Kaufman Hall analysis illustrates financial effects of inflation and the end of the COVID-19 public health emergency
CHICAGO – May 31ST, 2023 – Hospital finances broke even in April amid a continuing trend of high expenses and the unwinding of the Medicaid continuous coverage requirement of the COVID-19 public health emergency (PHE), according to the latest National Hospital Flash Report from Kaufman Hall.
Median YTD Operating Margin Shows Slight Improvement
The median year-to-date (YTD) operating margin index for hospitals was 0.0% in April, up slightly compared to -0.3% in March. With operating margins remaining at or below zero, hospitals have been left with little financial flexibility.
PHE Unwinding Begins
Hospitals experienced increases in bad debt and charity care in April. Combined with decreased patient volumes, Kaufman Hall experts note these data could illustrate the effects of the start of widespread disenrollment from Medicaid following the end of the PHE and the continuous enrollment provision that accompanied it. As states continue the process of redetermination, these trends will likely continue.
“With states conducting their Medicaid eligibility redetermination, it’s predicted that hundreds of thousands of people will ultimately become uninsured,” said Erik Swanson, senior vice president of Data and Analytics with Kaufman Hall. “The data indicate that we may already be seeing the effects of disenrollment materialize with patients less likely to seek out the care they need and a continued rise in bad debt and charity care.”
Inflation Pressures Hospital Finances
High expenses have been placing added strain on hospitals as they try to recover from the challenges of the pandemic. Labor expense per adjusted discharge increased 3% in April from March, and the costs of goods and services continued to be well above pre-pandemic levels. While total expenses fell slightly in April, operating revenues declined at a faster rate, down 5% month-over-month.
“Hospital and health system leaders must figure out how to navigate the new financial reality and begin to take action,” said Swanson. “In the face of operating margins that may never fully recover and inflated expenses, developing and executing a strategic path forward to a future that is financially sustainable is crucial.”
Kaufman Hallprovides management consulting solutions to help society’s foundational institutions realize sustained success amid changing market conditions. Since 1985, Kaufman Hall has been a trusted advisor to boards and executive management teams, helping them incorporate proven methods, rigorous analytics, and industry-leading solutions into their strategic planning and financial management processes, with a focus on achieving their most challenging goals.
Kaufman Hall services use a rigorous, disciplined, and structured approach that is based on the principles of corporate finance. The breadth and integration of Kaufman Hall advisory services are unparalleled, encompassing strategy; financial and capital planning; performance improvement; treasury and capital markets management; mergers, acquisitions, partnerships, and joint ventures; and real estate.
After three years of unprecedented challenges and caring for millions of patients, including over 6 million COVID-19 patients, America’s hospitals and health systems are facing a new existential challenge — sustained and significant increases in the costs required to care for patients and communities putting their financial stability at risk.
A confluence of several factors from historic inflation driving up the cost of medical supplies and equipment, to critical workforce shortages forcing hospitals to rely heavily on more expensive contract labor, led to 2022 being the most financially challenging year for hospitals since the pandemic began. Moreover, sustained demand for hospital care with patients coming to the hospital sicker and staying longer has exacerbated these challenges.
These challenges have been particularly financially devastating for hospitals and health systems because they come on top of two years of battling the COVID-19 pandemic. Hospitals and health systems have been on the front lines delivering care to patients, acting as de facto public health agencies, and incurring significant increases in costs from a range of inputs, including labor, drugs, supplies and administrative activities associated with burdensome billing and insurance tasks. In addition, as many individuals deferred care during the pandemic, hospitals saw a dramatic rise in patient acuity. At the same time, workforce shortages across the health care continuum have left hospitals unable to discharge patients to other care settings (e.g., skilled nursing facilities) creating patient bottlenecks with hospital beds occupied without any reimbursement.
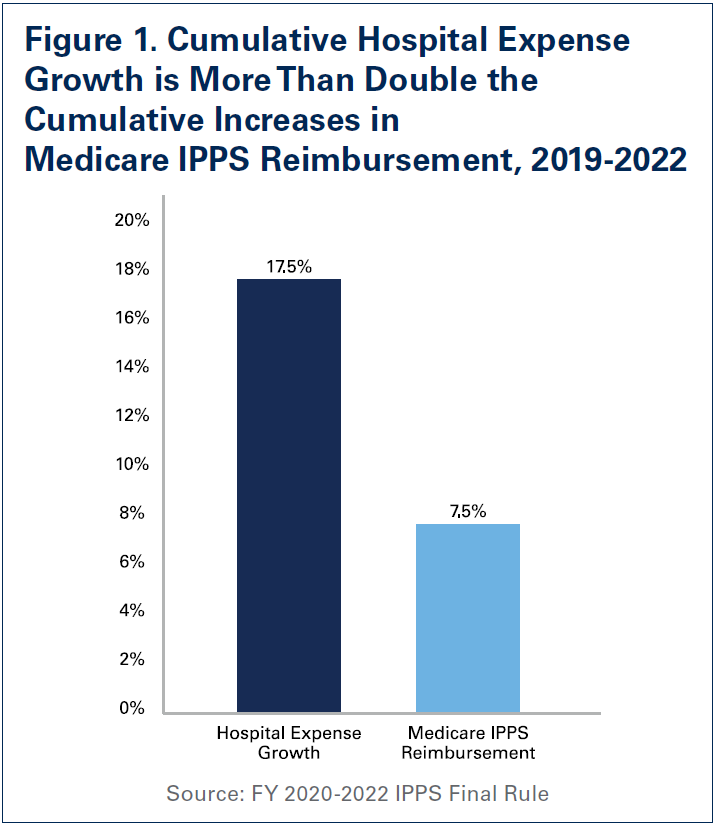
These unfortunate realities have resulted in a 17.5% increase in overall hospital expenses between 2019 and 2022, according to data from Syntellis Performance Solutions, a health care data and consulting firm. Further exacerbating the situation is the fact that the staggering expense increases have been met with woefully inadequate increases in government reimbursement. Specifically, hospital expense increases between 2019 and 2022 are more than double the increases in Medicare reimbursement for inpatient care during that same time (See Figure 1). Because of this, margins have remained consistently negative, according to Kaufman Hall’s Operating Margin Index throughout 2022 (See Figure 2). In fact, over half of hospitals ended 2022 operating at a financial loss — an unsustainable situation for any organization in any sector, let alone hospitals. So far, that trend has continued into 2023 with negative median operating margins in January and February. According to a recent analysis, the first quarter of 2023 saw the highest number of bond defaults among hospitals in over a decade.1 This also is one of the primary reasons that some hospitals, especially rural hospitals, have been forced to close their doors. Between 2010 and 2022, 143 rural hospitals closed — 19 of which occurred in 2020 alone.2,3 Finally, despite these cost increases, hospital prices have grown modestly. In fact, in 2022, growth in general inflation (8%) was more than double the growth in hospital prices (2.9%).
This report will examine the magnitude of cost increases over the last year, and the impact these increases have had on the financial stability of the hospital field.
Labor Expenses
Beginning in early 2022, the hospital field’s existing workforce shortages were exacerbated with increased patient demand for hospital care due to a combination of sustained COVID-19 surges, a new virulent disease affecting primarily pediatric patients called respiratory syncytial virus (RSV), and deferred care from the early days of the pandemic. To quickly meet this demand, hospitals were increasingly forced to turn to health care staffing agencies to fill necessary gaps, especially for bedside nursing and other critical allied health professionals such as respiratory and imaging technicians.
Labor has been really the primary driver of our increased expenses. We’ve seen a 17% increase in our nursing costs, for instance, during COVID, mainly because of many nurses leaving the field and the workforce. — President and CEO of a health system in the Northeast
A recent report by Syntellis Performance Solutions found that full-time equivalents (FTEs) for hospital contract employees jumped 138.5%. This reliance on temporary contract labor came at a significant expense to hospitals, as health care staffing agencies took advantage of the situation and increased their rates to record high levels. The same report found that the rate hospitals were charged for contract employees increased 56.8% in 2022 compared to pre-pandemic levels. It is for this reason that hospitals’ contract labor expenses increased a staggering 257.9% in 2022 relative to 2019 levels (See Figure 3).
The explosive growth in contract labor expenses in large part fueled the 20.8% increase in overall hospital labor expenses during the same time period. Even after accounting for the fact that patient acuity (as measured by the case mix index) has increased during this period, labor expenses per patient increased 24.7%. These increases are particularly challenging, because labor on average accounts for about half of a hospital’s budget.
Non-Labor Expenses
The historic rise in inflation has been particularly challenging for hospitals and health systems as it has sparked a significant increase in non-labor expenses. As prices for essential goods such as food and clothing have seen significant price growth, so too have the prices for essential goods for hospitals such as drugs and medical supplies.4 A report by Kaufman Hall estimated that non-labor expenses alone would result in a one-year expense increase of $49 billion for hospitals and health systems.5,6 In fact, since 2019, non-labor expenses have increased 16.6% on a per patient basis. Below, we focus on three areas of non-labor expenses that have seen tremendous cost growth:
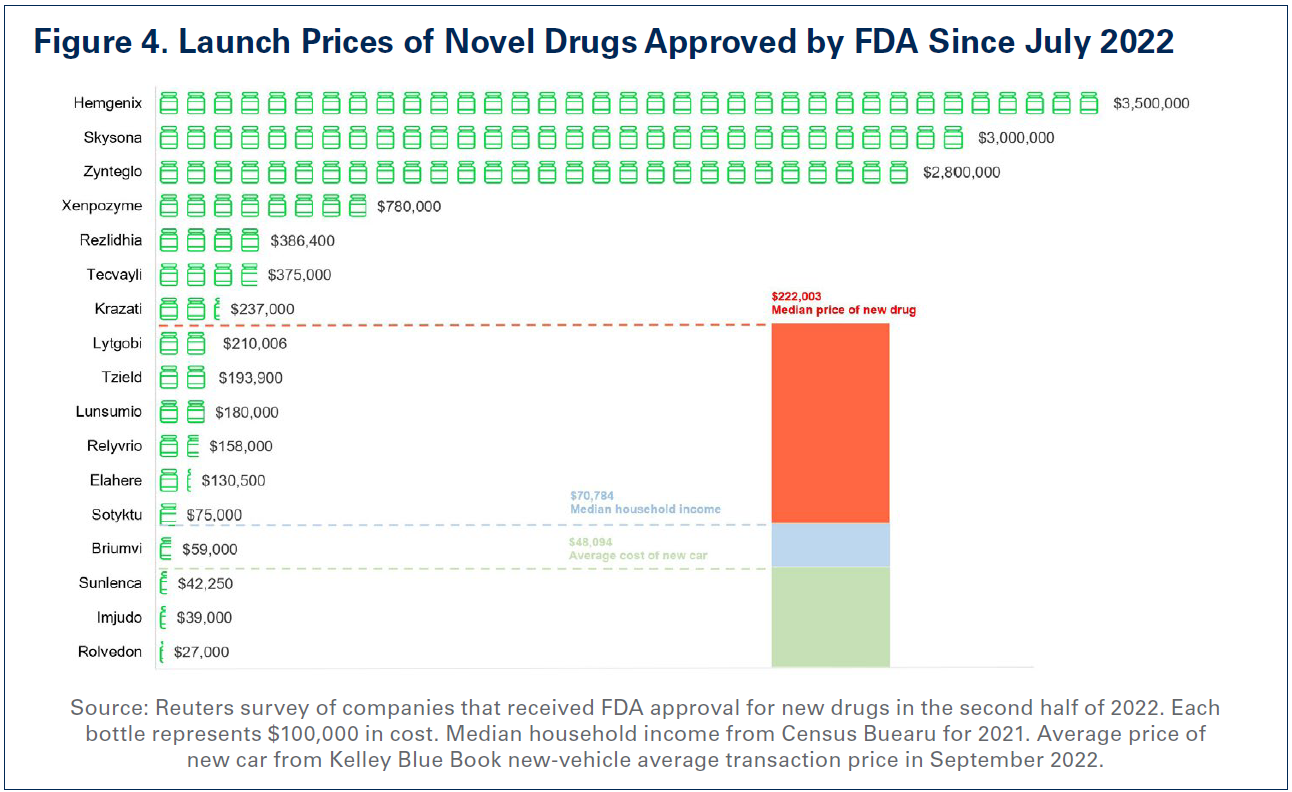
As hospitals and health systems faced an increasingly challenging environment due to pandemic surges as well as workforce shortages, drug companies took the opportunity to significantly raise the prices of existing drugs as well as introduce new drugs at record prices.7 High drug prices affect both patients directly and hospitals, especially when purchasing provider-administered drugs. In fact, for the first time in history, the median price of a new drug exceeded $200,000 — a staggering figure that implies a double-digit year-over-year price growth (See Figure 4).8,9 To further contextualize these launch prices, the median new drug launch price is more than quadruple the average price of a new car and more than triple the median annual household salary ($70,784) in the United States, illustrating how unaffordable these drugs are for both providers and their patients.10
In addition, a report by the Assistant Secretary for Planning & Evaluation (ASPE) at the Department of Health and Human Services (HHS) found that drug companies increased drug prices for 1,216 drugs — many used to treat chronic conditions like cancer and rheumatoid arthritis — by more than the rate of inflation, which was 8.5% between 2021 and 2022. In fact, the average price increase for these drugs was 31.6%, with some drugs experiencing price increases as much as 500%.11 Moreover, recent drug shortages, specifically for certain drugs used to treat cancer, have also fueled further expense growth. It is estimated that drug shortages alone cost hospitals nearly $360 million a year.12
Therefore, it is no surprise, that as hospitals face the reality of operating on negative margins, drug companies are enjoying record revenues and profits. For example, some drug companies are experiencing over 200% revenue growth.13
“In the last year, we’ve seen double digit increases in pharmaceuticals and medical supplies. Our utility costs are up and certainly our labor costs are up.” — CEO of a health system in the South
For these reasons, high drug prices have been a primary driver of skyrocketing drug costs for hospitals. According to data from Syntellis Performance Solutions, hospital drug expenses per patient have increased 19.7% between 2019 and 2022. Even after accounting for the fact that patients were on average sicker (as measured by the case mix index) in 2022 than in 2019, drug expenses per patient were up over 18%. This suggests that the growth in hospital drug expenses is not primarily due to sicker patients requiring more drugs, rather it is a result of drug companies’ deliberate decisions to increase the prices of their products.
II. Medical Supplies and Equipment
While the demand for patient care has risen, so has the need for medical supplies necessary to deliver patient care and personal protective equipment (PPE) necessary to ensure the safety of both hospital staff and patients. Hospitals rely on a global supply chain for access to these supplies and equipment, and entities across the supply chain have experienced inflationary cost increases. Ongoing supply chain disruptions have led to higher manufacturing costs, packaging costs, and shipping costs, which translate into higher prices for hospitals.14 In fact, the National Academies recently released a report highlighting the ongoing challenges that supply chain disruptions place on providers needing to access medical supplies.15
“But in other industries like we see in our area, manufacturing, retail, hospitality, you can decide not to fill that order. You can decide to shut your restaurant down for a day. We can’t do that in health care.” — President and CEO of a health system in the Midwest
As a direct result, hospital supply expenses per patient increased 18.5% between 2019 and 2022, outpacing increases in inflation by nearly 30%. Particularly alarming is the growth in supply costs needed for care in the emergency department — often the first level of care provided in the hospital. Hospital expenses for emergency services supplies experienced a nearly 33% increase between 2019 and 2022. These include equipment such as ventilators, respirators and other sophisticated equipment that are critical to keeping patients alive in the emergency department. As patient acuity has increased dramatically during this period, the need for these equipment to care for more complex patients also has increased.16 More specifically, as patients stay in the hospital longer requiring more intensive care, the amount of supplies and the type of supplies required to care for those patients become more expensive.17
III. Other Non-Labor Expenses
In addition to hospitals’ costs for drugs and medical supplies and equipment, costs for other areas that help support patient care such as purchased service expenses also have risen precipitously. This, in part, has driven clinical costs higher, making clinical services such as emergency and lab services more expensive to administer.
Purchased service expenses, which are expenses hospitals incur to create operational efficiencies such as information technology (IT), environmental services and facilities, and food and nutrition services increased 18% between 2019 and 2022. With increased patient demand and inflationary pressures, hospitals have been forced to incur additional purchased service costs as they renew and renegotiate their purchased service contracts. For example, as the cost of food has gone up over the last year, hospitals’ food services costs have grown. Specifically, food and nutrition service expenses per patient grew over 15% between 2019 and 2022.
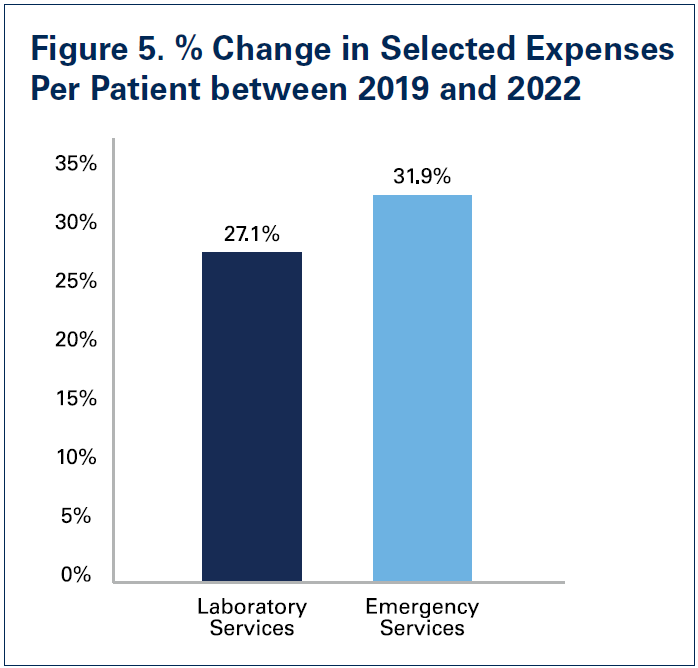
Hospitals also have incurred increased costs in particular clinical areas. This is due to a combination of increased patient demand after many patients delayed or avoided care during the pandemic and inflationary cost growth for supplies and equipment needed to provide care. Specifically, compared to 2019 levels, laboratory service expenses per patient were up 27.1% in 2022 and emergency service expenses per patient were up 31.9%.
With hospitals bearing cost growth in many areas, they have been forced to cut costs elsewhere to stay financially afloat, and in the case of many rural hospitals, simply keep the doors open.
Expenses from Burdensome Insurer Policies
Notwithstanding labor and non-labor expense increases, commercial health insurer policies like unnecessary prior authorization requirements and improper claim denials continue to add significant burden for hospital staff — diverting staff time from caring for patients and contributing to clinician burnout. These practices add substantial administrative costs to the health care system by slowing down the provision of care, requiring providers to purchase additional IT tools to manage insurer requirements and necessitating the hiring of additional staff solely to manage administrative paperwork.
Administrative costs constitute as much as 31% of total health care spending — 82% of which can be attributed to billing and insurance.18 In a recent survey fielded by the AHA, 84% of hospitals reported the cost of complying with insurer policies is increasing, with 95% reporting increases in time spent seeking prior authorization approval.19 Even though more than half of all prior authorization denials are overturned, commercial health insurers continue to flood hospitals with prior authorization denials to the detriment of both patients and providers. This is especially egregious when prior authorization is required for widely available lifesaving medications with clear clinical indications for use, such as insulin, where the service or treatment protocol are neither new nor have a history of unwarranted variation in utilization. The AHA report also found that 50% of hospitals and health systems have more than $100 million in accounts receivables for claims that are older than six months, which impact hospitals’ cash flow and ability to weather the avalanche of cost increases they have faced. Shockingly, seven in 10 hospitals reported having an outstanding claim from 2016 or older. In addition, 35% of hospitals reported $50 million or more in foregone payments because of denied claims.
A recent survey conducted by Morning Consult on behalf of the AHA found that nearly three-fourths of nurses reported increases in insurer-required administrative tasks for medical services over the last five years. Nearly 9 in 10 nurses reported insurer administrative burden had negatively impacted patient clinical outcomes (See Figure 6 on next page).
Confronted by ever-growing costs, hospitals have been limited in how they can respond to the administrative burden levied by commercial health plans. Over the course of the last several years many hospitals, looking for operational efficiencies to combat rising costs, have been driven to trim down their administrative workforce.20 However, with a narrowing menu of options for hospitals to choose from in responding to insurer administrative expenses, 78% of hospitals report their experience with commercial health insurers is getting worse.
Outlook for the Rest of 2023
As the public health emergency comes to end on May 11, a number of important waivers and flexibilities also will come to an end immediately, or will sunset at the end of this year.21 The downstream effects of this will be wide-ranging as hospitals will be faced with a set of additional challenges. For example, with the end of the public health emergency, the continuous Medicaid enrollment provision will no longer be in effect starting April 1 meaning that states can begin dis-enrolling current Medicaid beneficiaries from the program that do not meet the state’s Medicaid enrollment criteria. According to the Kaiser Family Foundation, as many as 14 million current Medicaid beneficiaries could lose coverage over the next year.22 Undoubtedly, these coverage losses will drive higher rates of uninsured and underinsured individuals, raising hospitals’ uncompensated care costs and potentially negatively impacting disproportionate share payments as well as 340B program eligibility, both of which allow hospitals to offset some of the expense increases as well as furnish programs and services critical to patients. Further, the ending of regulatory relief through the 20% Medicare inpatient prospective payment system add-on payment for beneficiaries diagnosed with COVID-19 to offset the cost of highly complex care for these patients, will certainly add financial pressure to an already fragile situation for hospitals and health systems.
The combination of the impacts on hospitals of the ending public health emergency as well as continued expense growth has created an uncertain future for hospitals and health systems. A study by McKinsey on the impact of inflation and other cost pressures for the health care system projected that there would be $98 billion in additional costs between 2022 and 2023 alone, representing an astounding $248 billion increase in costs relative to 2019.23 In fact, their projections suggest that non-labor costs alone could increase by $112 billion by 2027. Therefore, it is no surprise, that credit rating agencies have a negative outlook for the field. For example, Moody’s has projected a negative outlook for the hospital field for 2023 due in large part to inflationary cost pressures and persisting workforce challenges.24
Conclusion
Hospitals and health systems — and their teams — are committed to providing high-quality care to all patients in every community. This steadfast commitment to caring and advancing health has never been more apparent than during the last three years battling the greatest public health crisis in a century.
However, the costs of delivering on this commitment to care have grown tremendously. As the data in this report show, 2022 brought an unprecedented set of challenges for hospitals and health systems, which has left the field in a financially unsustainable situation. These challenges are continuing in 2023.
To address these challenges and ensure hospitals have the ability to continue taking care of the sick and injured, as well as keeping people and communities healthy, congressional support and action are necessary. Among other actions, Congress should:
enact policies that bolster hospitals and health systems’ efforts to support today’s workforce and ensure a future pipeline of professionals to mitigate longstanding workforce challenges and meet the nation’s increasing demands for care;
reject efforts to cut any Medicare or Medicaid payments to hospitals and health systems. Medicare and Medicaid significantly underpay the costs of providing care and further cuts could reduce access to care for patients and communities;
establish a temporary per diem payment to address a backlog in hospital patient discharges due to workforce shortages;
urge the Centers for Medicare & Medicaid Services to use its “special exceptions and adjustments” authority to make a retrospective adjustment to account for the difference between the market basket update that was implemented for fiscal year (FY) 2022 and what the market basket is currently projected to be for FY 2022; and
create a special statutory designation and provide additional support for metropolitan anchor hospitals that serve historically marginalized communities.
As the hospital field maintains its commitment to care in the face of significant challenges, policymakers must step up and help protect the health and well-being of our nation by ensuring America has strong hospitals and health systems.
The American Hospital Association released a report in April examining the costs that drove 2022 to be a financial low point for hospitals and health systems.
The AHA’s “Cost of Caring” report contains percent changes for a number of expense categories from 2019 to 2022, with data from consulting firm Syntellis Performance Solutions. It concludes with five suggestions from the association to Congress for action and greater support, including the rejection of any efforts to cut Medicare and Medicaid reimbursement.
“Rising costs for drugs, supplies, and labor coupled with sicker patients, longer hospital stays and government reimbursement rates that do not come close to covering the costs of caring for patients have created a dire situation for hospitals and health systems,” AHA President and CEO Rick Pollack said in the report. “This is not just a financial problem, it is an access problem. When healthcare providers cannot afford the tools and teams they need to care for patients, they will be forced to make hard choices and the people who will be impacted the most are patients. We can’t let that happen. Congress and others must act to preserve the care our nation needs and depends on.”
Below are some key figures from the report, which can be found in full here.
1. Overall hospital expenses increased by 17.5 percent from 2019 to 2022, according to data from consulting firm Syntellis Performance Solutions. By comparison, Medicare reimbursement increased 7.5 percent in the same timeframe.
2. Overall hospital labor expenses increased 20.8 percent from 2019 to 2022, with labor expenses per patient up 24.7 percent.
3. Temporary contract labor was a significant expense within the labor category throughout the COVID-19 pandemic. Total contract labor expenses for hospitals in 2022 were 258 percent higher than in 2019. The rate hospitals were charged for contract employees increased 56.8 percent in 2022 compared to pre-pandemic levels.
4. Drugs make up another large expense category for hospitals, which have seen a 19.7 percent increase in drug expenses per patient between 2019 and 2022. This measure exceeds 18 percent when accounting for patient case mix and acuity, suggesting the increase stems from drugmakers’ pricing strategies.
5. Purchased service expenses — for operational functions such as IT, environmental services and facilities, and food and nutrition services — increased 18 percent between 2019 and 2022.
6. Hospital supply expenses per patient increased 18.5 percent between 2019 and 2022. Emergency departments were especially hard-hit by supply costs, which grew 33 percent between 2019 and 2022.
7. Food and nutrition service expenses per patient increased 15 percent between 2019 and 2022.
8. Laboratory service expenses per patient increased 27.1 percent between 2019 and 2022. Emergency service expenses per patient grew 31.9 percent in the same timeframe.
Some drug shortages have worsened because of the closure of Gurnee, Ill.-based Akorn Operating Co., according to the American Society of Health-System Pharmacists.
Major hospital groups are ramping up resistance to physician-owned hospitals, which were checked by the Affordable Care Act but have recently become subject of renewed attention.
Physician-owned hospitals have been largely quiet in conversations about hospitals over the past decade-plus due to the Affordable Care Act. Enacted in 2010, the law placed a number of restrictions on POHs, including a prohibition on expanding the capacity of existing Medicare-certified POHs unless they meet certain exceptions and a moratorium on the establishment of new Medicare-certified POHs.
In December 2022, POHs regained some industry attention when CMS granted a “high Medicaid facility” expansion request from Edinburg, Texas-based Doctors Hospital at Renaissance to establish a new physician-owned hospital 55 miles away in Brownsville.
The Federation of American Hospitals, which represents investor-owned hospitals, heavily criticized the development as unlawful and argued that the 55-mile distance between DHR’s main campus and new location makes it “a thinly veiled attempt to set up a new POH in a new service area.”
Shortly after that development, in February, more than a dozen Republican lawmakers reintroduced legislation that would repeal the ACA’s ban on POHs. The bill, dubbed the Patient Access to Higher Quality Health Care Act, received support from the American Medical Association and Physician-Led Healthcare for America.
“The hospital industry has long argued that physicians cherry-picked healthy patients and preferred those with private insurance as a rationale for supporting the ban on physician-owned hospitals,” legislation co-sponsor Sen. James Lankford, R-Okla., co-authored with an assistant professor of Medicine at the Johns Hopkins University School of Medicine in an op-ed for The Wall Street Journal, likening the ban on physician-owned hospitals to the absurdity of a ban on chef-owned restaurants.
Now, a new report jointly issued by the FAH and American Hospital Association reasserts the idea that POHs cherry pick. The March 23 report, prepared by health economics and policy consulting firm Dobson DaVanzo & Associates, suggests POHs are outliers compared to their non-POH counterparts due in large part to their patient populations and acuity.
Based on an analysis of 163 POHs and 3,020 non-POHs, the report contends that POHs generally treat a population that is younger, less complex or comorbid, and less likely to be dually eligible or non-white, the report states. They also have higher margins and lower unreimbursed and uncompensated care costs as a percent of net patient revenue compared to non-POHs.
“If there was ever any doubt, the evidence against POHs is as crystal clear today as it was when Congress passed the self-referral ban in 2010,” FAH President and CEO Chip Kahn said in a statement. “Weakening or unwinding the current ban opens the door further to the very behaviors that Congress sought to prevent.”
“The growth of physician-owned hospitals was restricted by Congress for good reasons and those remain valid today as this analysis shows,” AHA President and CEO Rick Pollack said in a statement. “Physician-owned hospitals undermine our nation’s health care safety-net and jeopardize access to care by cherry-picking the most profitable cases and avoiding patients with complex conditions and lower-reimbursing coverage.”
Texas regulators have placed Friday Health into liquidation and ordered the company to end all business in the state.
A district court in Austin found that Friday’s Texas subsidiary was insolvent and had not maintained a minimum surplus of $1.4 million under state law, according to regulatory filings dated March 23.
Texas Insurance Commissioner Cassie Brown has been appointed to liquidate and take possession of the company’s remaining operations in the state, including all physical, financial and digital assets. Ms. Brown is also authorized to direct and manage Friday employees and terminate them at her discretion.
Law firm Cantilo & Bennett is now in control of day-to-day operations in Texas, though the state said most policies have expired. Any remaining claims will be paid by the Texas Life and Health Insurance Guaranty Association, meaning health plans in Texas could be financially impacted.
As of May 2022, Alamosa, Colo.-based Friday Health Plans had 330,000 members across seven states and an estimated $1.95 billion in 2022 revenue.
“This development in Texas does not impact our business or operations in any other states,” the company wrote on its website. “We remain committed to our mission to provide simple, high-quality, affordable and easy-to-use insurance to our growing membership.”
Last fall, Texas asked Friday to leave the state’s ACA marketplace for 2023 following operational challenges. The company also pulled out of the New Mexico exchange.
Friday is also laying off 98 workers in Alamosa and Denver on April 30 due to a “loss of business,” according to state filings.
The company was founded in 2015 and offers individual and small group plans both on and off the exchange. In 2023, the company is offering ACA plans in Colorado, North Carolina, Georgia, Nevada and Oklahoma.
Friday’s CEO is Beth Bierbower, Humana’s former president of group and specialty benefits. The company’s CFO is Rhonda Bagby, who was most recently vice president of finance and commercial at Bright Health.
Hospital finances are starting to stabilize as razor-thin margins become the new normal, according to Kaufman Hall’s latest “National Flash Hospital Report,” which is based on data from more than 900 hospitals.
External economic factors including labor shortages, higher material expenses and patients increasingly seeking care outside of inpatient settings are affecting hospital finances, with the high level of fluctuation that margins experienced since 2020 beginning to subside.
Hospitals’ median year-to-date operating margin was -1.1 percent in February, down from -0.8 percent in January, according to the report. Despite the slight dip, February marked the eight month in which the variation in month-to-month margins decreased relative to the last three years.
“After years of erratic fluctuations, over the last several months we are beginning to see trends emerge in the factors that affect hospital finances like labor costs, goods and services expenses and patient care preferences,” Erik Swanson, senior vice president of data and analytics with Kaufman Hall, said. “In this new normal of razor thin margins, hospitals now have more reliable information to help make the necessary strategic decisions to chart a path toward financial security.”
High expenses continued to eat into hospitals’ bottom lines, with February signaling a shift from labor to goods and services as the main cost driver behind hospital expenses. Inflationary pressures increased non-labor expenses by 6 percent year over year, but labor expenses appear to be holding steady, suggesting less dependence on contract labor, according to Kaufman Hall.
“Hospital leaders face an existential crisis as the new reality of financial performance begins to set in,” Mr. Swanson said. “2023 may turn out to be the year hospitals redefine their goals, mission, and idea of success in response to expense and revenue challenges that appear to be here for the long haul.”
Twenty-four hospitals in the U.S., Canada and Western Europe are using “black boxes” — named after the recording devices in airplanes — to collect and analyze operating-room practice data in hopes of reducing medical errors and improving patient safety and operating room efficiency, The Wall Street Journal reported March 19.
The OR Black Box, made by Surgical Safety Technologies in Toronto, gathers video, audio, patient vital signs and data from surgical devices during surgery. Audio and video are deidentified, giving participants blurred faces and cartoonish bodies, according to the report. Hospitals can use the data to view performance over time or to analyze particular operations.
Mayo Clinic has used the device in three operating rooms over the last year in order to improve surgical safety and outcomes, according to Susan Hallbeck, PhD, professor of healthcare systems engineering at Rochester, Minn.-based Mayo Clinic’s Kern Center for the Science of Health Care Delivery.
Durham, N.C.-based Duke University Hospital has installed OR Black Boxes in two operating rooms to study and improve patient positioning to reduce skin tissue and nerve injuries and to improve communication among nurse personnel during surgical procedures. The boxes have helped the system identify a need for a better sending and tracking system for specimens, Rebecca McKenzie, DNP, RN, assistant vice president for perioperative services at Duke University Hospital, told the Post. The Duke teams have also found new ways to increase operating room efficiency and productivity by reducing the amount of time to prepare an operating room for the next procedure. The health system is considering using the box as a teaching tool for nurses’ OR training, she said.
The University of Texas Southwestern Medical Center in Dallas is using five black boxes to understand the characteristics of a high-performing operating room team.
However, some worry the black boxes could be used to assign blame and punishments.
“Aggregate data is deidentified and anonymized so we can learn from it now and in the future, and audiovisual data is deleted after 30 days to protect the privacy and confidentiality of patients and healthcare providers,” Surgical Safety Technologies founder Teodor Grantcharov, MD, PhD, a professor of surgery and practicing surgeon at Stanford Medicine, said in the article.
Others worry the information could be used in lawsuits; however, there has not yet been a case where this information was requested or used in court.
The anonymization of information from the OR Black Box makes it unlikely to be used in malpractice litigation, David Feldman, MD, chief medical officer at Healthcare Risk Advisors, a New York City-area company working with hospitals on how to reduce malpractice risk, said in the report.
“I believe it will make surgery safer and thus reduce liability and malpractice claims,” he said.
About 40 hospitals across five states have filed a lawsuit against HHS Secretary Xavier Becerra, alleging that yearslong delays in correcting Medicare disproportionate share hospital payments have cost them “tens of millions” of dollars.
The safety-net hospitals in California, Arizona, Nevada, Hawaii and Minnesota filed the lawsuit March 14 in a Washington, D.C., district court.
DSH payments are meant to support hospitals that have a high mix of low-income patients. In 2008, a federal court in Washington, D.C., ruled against how HHS calculates the payments and ordered the government to send payments to its contractors to determine how much was still owed to the hospitals.
“The agency’s contractors have not performed the revised determinations required under the ruling and the rule and have not paid the plaintiff hospitals any of the additional amounts due them for the periods at issue,” the lawsuit alleges.
In 2010, HHS revised the process it uses to calculate DSH payments and said it would correct identified errors, but the hospitals allege there have been delays in the amended payments.
“The agency’s unreasonable delay has cost the plaintiff hospitals tens of millions of dollars in funds that should have been paid to them many years ago for the higher costs that they incurred to treat low-income patients more than a decade ago,” the plaintiffs’ attorneys wrote.
In 2020, CMS instructed Medicare contractors to halt efforts to settle cost reports, saying they had not yet completed the appropriate public notification process. Medicare contractors were told not to take further action “until expressly instructed by CMS,” according to court documents obtained by Becker’s.
The plaintiffs are seeking reimbursement from HHS via revised payment determinations — reflecting additional DSH amounts as a result of recalculated SSI fractions — plus interest and legal costs.
The lawsuit also alleges that HHS is using another lawsuit, Azar v. Allina Health Services, as a reason for “unreasonably” delaying and “unlawfully” withholding payments.
More than 20 of the plaintiffs are affiliated with San Francisco-based Dignity Health. Becker’s has reached out to Dignity Health and HHS for comment and will update this article if more information becomes available.
The first hospitals seeking CMS’ new rural emergency hospital designation have submitted their applications, Kaiser Health News reported March 6.
Hospitals that convert receive a 5 percent increase in Medicare payments as well an average annual facility fee payment of about $3.2 million, according to the report. In return, the hospitals must close their inpatient beds and focus solely on outpatient and emergency care.
The hospitals showing immediate interest have three or fewer patients staying overnight at any given time and have typically given up maternity care long ago to save on expenses, according to the report.
One hospital in the Stillwater (Okla.) Medical system — an outpost in Perry, Okla. — has already applied for the designation, according to the report. Another in Blackwell, Okla., will likely do the same.
Stillwater Medical Chief Administrative Officer Steven Taylor said the switch makes sense for the two hospitals that have struggled financially, according to the report. He said the most important thing for the small communities where the hospitals are located is to keep emergency services.
Guadalupe County Hospital in Santa Rosa, N.M., is another that has already applied for the designation, according to the report. Despite the help of a tax levy, the hospital has lost more than $1 million in the past six months.
“For years, we’ve been anticipating kind of our own demise, praying that a program would come along and make us sustainable,” Guadalupe County Hospital Administrator Christina Campos told the outlet.
A two-bed facility in Crosbyton, Texas, recently became the first in the state to get approval for the new designation. John Henderson, president and chief executive of the Texas Organization of Rural & Community Hospitals, told the outlet that several more of the state’s 158 rural hospitals have applied, are applying or are considering the conversion.

 These challenges have been particularly financially devastating for hospitals and health systems because they come on top of two years of battling the COVID-19 pandemic. Hospitals and health systems have been on the front lines delivering care to patients, acting as de facto public health agencies, and incurring significant increases in costs from a range of inputs, including labor, drugs, supplies and administrative activities associated with burdensome billing and insurance tasks. In addition, as many individuals deferred care during the pandemic, hospitals saw a dramatic rise in patient acuity. At the same time, workforce shortages across the health care continuum have left hospitals unable to discharge patients to other care settings (e.g., skilled nursing facilities) creating patient bottlenecks with hospital beds occupied without any reimbursement.
These challenges have been particularly financially devastating for hospitals and health systems because they come on top of two years of battling the COVID-19 pandemic. Hospitals and health systems have been on the front lines delivering care to patients, acting as de facto public health agencies, and incurring significant increases in costs from a range of inputs, including labor, drugs, supplies and administrative activities associated with burdensome billing and insurance tasks. In addition, as many individuals deferred care during the pandemic, hospitals saw a dramatic rise in patient acuity. At the same time, workforce shortages across the health care continuum have left hospitals unable to discharge patients to other care settings (e.g., skilled nursing facilities) creating patient bottlenecks with hospital beds occupied without any reimbursement.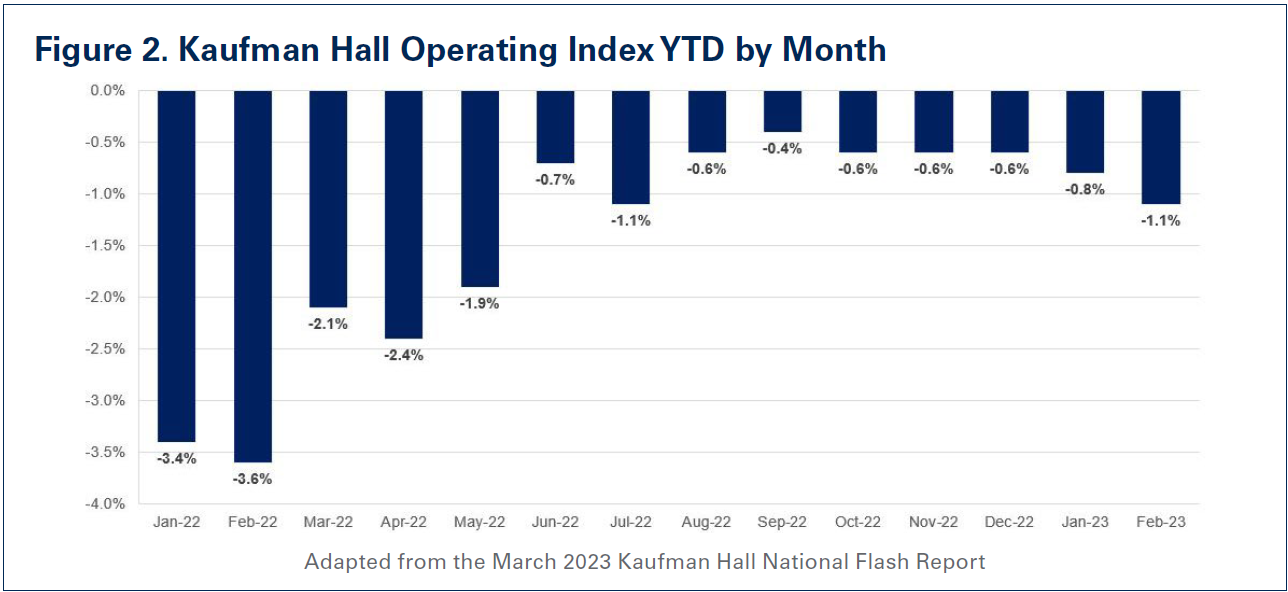
 In addition to hospitals’ costs for drugs and medical supplies and equipment, costs for other areas that help support patient care such as purchased service expenses also have risen precipitously. This, in part, has driven clinical costs higher, making clinical services such as emergency and lab services more expensive to administer.
In addition to hospitals’ costs for drugs and medical supplies and equipment, costs for other areas that help support patient care such as purchased service expenses also have risen precipitously. This, in part, has driven clinical costs higher, making clinical services such as emergency and lab services more expensive to administer.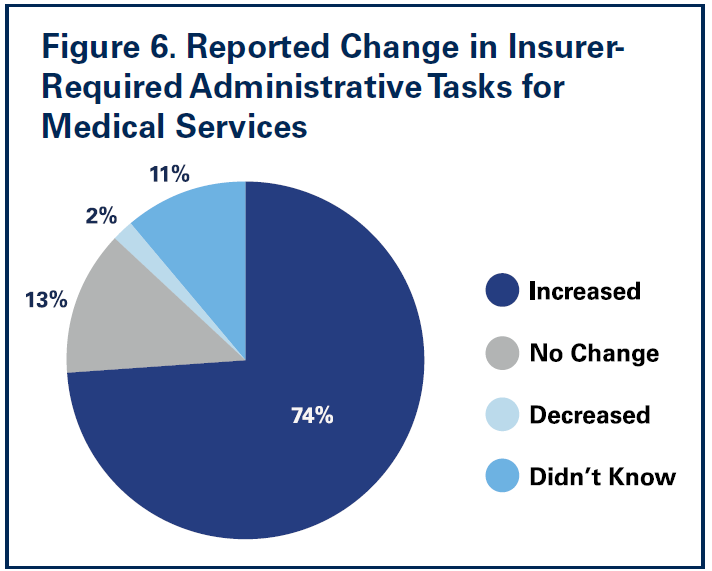 A recent survey conducted by Morning Consult on behalf of the AHA found that nearly three-fourths of nurses reported increases in insurer-required administrative tasks for medical services over the last five years. Nearly 9 in 10 nurses reported insurer administrative burden had negatively impacted patient clinical outcomes (See
A recent survey conducted by Morning Consult on behalf of the AHA found that nearly three-fourths of nurses reported increases in insurer-required administrative tasks for medical services over the last five years. Nearly 9 in 10 nurses reported insurer administrative burden had negatively impacted patient clinical outcomes (See