21.9% increase in supply expense (not including purchased services or pharmaceuticals) for hospitals from September 2021 to September 2022.1 During this same period, Kaufman Hall reports that purchased services expenses increased 16.2%.
Hospitals have faced a $11,950 supply cost increase per bed in 2022.2 This amounts to an average increase in supply expense of about $330 per admission, and a 6.2% increase per discharge.
19% The cost decrease for patients treated at home versus an inpatient hospital setting.3
24 hospitals and health systems launched innovation centers in 2021.4 How are suppliers and supply chain going to participate?
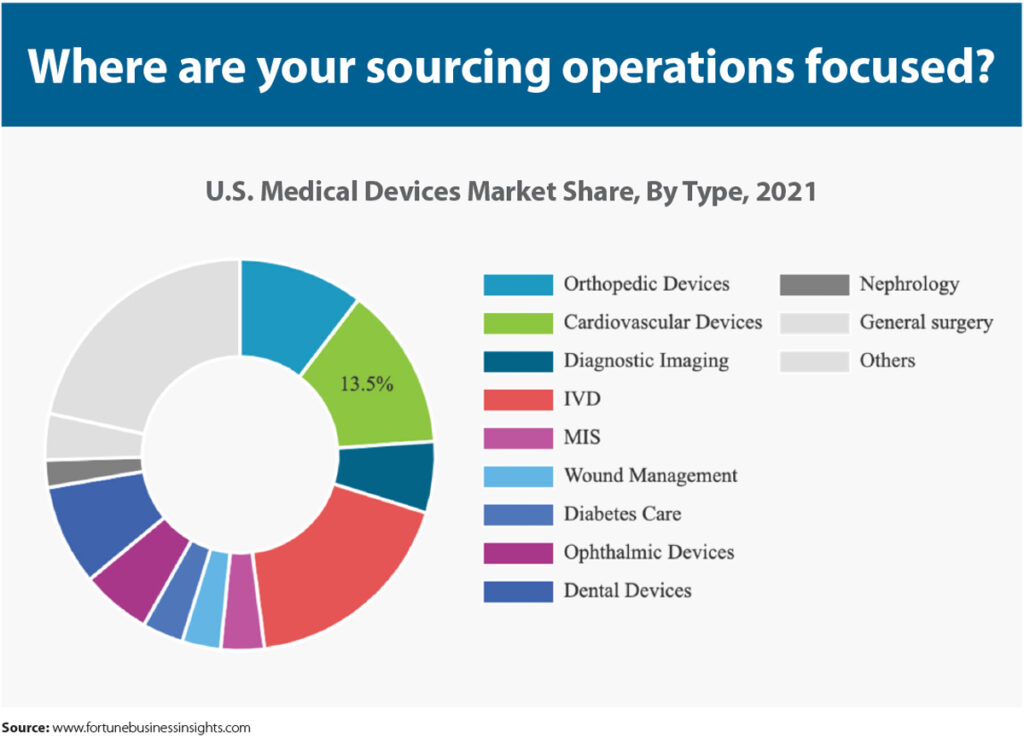
By 2030, more than 50% of joint replacements will be performed in ambulatory Surgery Centers (ASCs)5. 21% of the typical ASC is presently for orthopedic procedures.6
0 The number of container ships waiting to dock at the Port of Los Angeles on December 2, 2022.
The number of supply shortages are now roughly 5x the number in 2019, according to a recent Premier, Inc. study.
5.8% The decrease in quarterly active drug shortages between Q1 2019 and Q3 2022.7 (276 vs. 260).
Hospitals and Health Systems joining the Health Sector Climate Pledge has reached 1,000. Meanwhile, 71% of healthcare environmental emissions come from supply chain related activities, according to Greenhealth Exchange.
Politically driven healthcare supply chain waste during COVID is monumental8
40,000 Initial estimate by the State of New York on the number of ventilators needed to fight COVID.
8,555 Actual number of ventilators purchased by NY state, for $166M along with 1,179 X-Ray machines for $86.4M. 2,141 ventilators had been deployed as of September 2022.
200,000 Ventilators ordered by the Trump administration in 2020 for $3B, but only 50% “had the capacity to support the most severely affected patients.”
$633M Cost of at-home COVID-19 tests from a political contributor to New York Governor Kathy Hochul.
1 Kaufman Hall “National Hospital Flash Report”, September, 2022
2 Computed from Kaufman Hall Op. Cit. and American Hospital Association Data.
Last year brought its share of challenges. Finding solutions is the hard work awaiting everyone in the healthcare community this year.
February 2023 – The Journal of Healthcare Contracting
2022 presented all kinds of challenges for providers, patients and public health professionals. No doubt many of those challenges will linger in 2023, and new ones will arise. However, researchers, providers, public health professionals, lawmakers – and supply chain leaders – can be expected to keep working through the tough issues facing them. In the first part of a series, JHC examines the following issues:
Respiratory season
Monkeypox
Respiratory season: In like a lion
Predictions of a tumultuous respiratory season – fueled by COVID-19, influenza and respiratory syncytial virus – appeared to be coming true at year’s end. Will any of the public-health-related measures society learned during the pandemic ease the damage?
In November, the Centers for Disease Control and Prevention (CDC) reported that early increases in seasonal influenza activity were continuing nationwide, with the Southeast and South-Central areas of the country hardest hit. The agency estimated that as of Nov. 1, influenza accounted for 1.6 million illnesses, 13,000 hospitalizations and 7,300 deaths (including two pediatric deaths), and the cumulative hospitalization rate was higher than the rate observed in week 43 during every previous season since 2010-2011.
In addition to elevated levels of flu, CDC was tracking rises in respiratory syncytial virus (RSV), Rhino viruses and animal viruses. Children’s hospitals were overflowing with RSV patients.
Long COVID
Although the incidence of COVID-19 had abated by late 2022, the healthcare community still faced a challenging after-effect – Long COVID. Between 7.7 million and 23 million people in the United States could have Long COVID, whose symptoms can linger for weeks, months and even years, according to U.S. government estimates.
The most reported symptoms include fatigue, symptoms that worsen after physical or mental effort, fever, and lung (respiratory) symptoms, including difficulty breathing or shortness of breath and cough.
People who had suffered severe illness with COVID-19 were more likely to experience organ damage affecting the heart, kidneys, skin and brain. Abnormalities of the thyroid joined the ever-growing list of side effects attributed to Long COVID, according to research presented at the American Thyroid Association 2022 Annual Meeting in October. Inflammation and problems with the immune system were also said to occur. Effects such as these could lead to the development of new conditions, such as diabetes or a heart or nervous system condition, according to Mayo Clinic.
At year’s end, researchers were still questioning whether Long COVID is a new syndrome and unique to COVID-19. That’s because some symptoms are similar to those caused by chronic fatigue syndrome and other chronic illnesses that develop after infections. Despite the questions, however, the healthcare community continued to learn more about Long COVID, how to treat it, and even how to prevent it.
For example, in November, the U.S. Department of Veterans Affairs released a study showing the medication Paxlovid can reduce the risk of symptoms of Long COVID. The study, which included more than 56,000 veterans with a positive SARS-CoV-2 test, showed that those given the oral antiviral medication in the first five days of a COVID-19 infection had a 25% decreased risk of developing 10 of 12 different Long COVID conditions studied, including heart disease, blood disorders, fatigue, liver disease, kidney disease, muscle pain, neurocognitive impairment and shortness of breath.
Monkeypox: Lessons learned about ‘stigma’ disease
Monkeypox cases were declining by year’s end, but some observers believe progress could have been swifter.
In the U.S., about 27,635 cases were reported in late October, about 85% down from the peak at the outbreak, reported Demetre Daskalakis, MD, White House National Monkeypox Response deputy coordinator. However, he added, “the outbreak is really concentrated in communities of color, specifically among Black individuals.”
The CDC reported on a clinical consultation for 57 hospitalized patients with severe manifestations of monkeypox, most of whom were Black men with AIDS. Delays had been observed in initiation of monkeypox-directed therapies. Twelve patients died, and monkeypox was a cause of death or contributing factor in five patients to date, with several other deaths still under investigation.
As a result, CDC advised clinicians to consider early treatment with available therapeutics for those at risk for severe monkeypox disease, particularly patients with AIDS. Engaging all persons with HIV in care remains a critical public health priority.
According to one U.S. epidemiologist, the monkeypox experience demonstrated that the world has made little progress since the 1980s AIDS epidemic. “As with the AIDS epidemic, sluggish responses from governments and international institutions, plus outright homophobia and bureaucratic bumbling, have hampered efforts to contain the outbreak,” wrote Gregg Gonsalves, an epidemiologist at the Yale School of Public Health in New Haven, Connecticut, in a commentary in Nature. “Very often, humanity has the ability to prevent and treat infectious disease; not doing so is a political choice.”
That said, public health officials around the world were applying lessons learned from the AIDS epidemic to monkeypox. “Local staff in the most affected states [in Nigeria] have reported that stigma, connected with commentary from across the world blaming gay people for monkeypox, is discouraging some people from seeking care,” said Dr Leo Zekeng, UNAIDS Country Director and Representative in Nigeria in August. “State Health officials are working to ensure that staff at health clinics are sensitized to break down such stigma, and not to reinforce it. State Ministry of Health officials are also embarking on community sensitization on monkeypox, emphasizing identification of symptoms, prevention and the need to get tested.”
In September, the U.S. FDA made a significant step forward in early detection of monkeypox by authorizing emergency use of in vitro diagnostics for the detection or diagnosis of monkeypox. These diagnostics may detect the monkeypox virus specifically or more generally detect non-variola orthopoxviruses, which include monkeypox virus.
Supply chain friction is here to stay, in one form or another. Recently, congestion has eased at our nation’s seaports, with fewer delays at cargo terminals. But as one set of disruptions have eased, other challenges have emerged to their place.
Labor Issues
In December, HIDA urged Congress to take steps to maintain the freight rail system and avert any rail strike. As Americans weathered a difficult flu season and a surge in pediatric RSV cases, it was no time to disrupt the medical supply chain. The consequences would have been dire, with the potential to impede the delivery of medical products needed to treat patients, protect providers, and save lives. HIDA urged President Biden to take action to avert a rail strike. Fortunately, Congress intervened in a bipartisan fashion and passed legislation to settle the labor dispute and keep the supply chains moving. However, attention will now focus on the current labor negotiations at the West Coast ports.
Fuel Shortages
Although the cost of gasoline has come down from last year’s peak, the price of diesel fuel has remained stubbornly high. This autumn, diesel fuel supplies fell to their lowest level since the U.S. government started keeping records in 1982. Limited refinery capacity and the Russian invasion of Ukraine have contributed to price increases. Separately, a directive from the International Maritime Organization two years ago to require most oceangoing ships to replace their high-sulfur bunker fuel with less polluting fuels, which has slowly increased demand for diesel. Energy analysts estimate that the global shipping fleet was now consuming half a million barrels of diesel a day, or roughly 2% of the world’s supplies.
Unpredictable and Fragile Supply Chains
According to research from The Advisory Board, healthcare providers are facing long-term shortages of medical products and greater unpredictability in the supply chain. More than 90% of provider executives report that they are still experiencing product shortages. Every link in the supply chain is potentially fragile. In the last three years, we’ve seen bottlenecks in air freight, shipping, trucking and rail. Distributors have shown great resourcefulness and resolve to overcome the multitude of challenges they have faced.
HIDA continues to work with supply chain experts among our member companies to monitor shipping and transportation trends. We facilitate meetings with port officials and federal agencies to resolve bottlenecks. We know that transportation is a healthcare issue, and continue to focus on long-term solutions to create a “fast pass” system to expedite critical products so patients and providers can get the medical supplies they need.
Linda Rouse O’Neill, Vice President, Supply Chain Policy and Executive Branch Relations, Health Industry Distributors Association
The Biden administration has informed Congress it will end the COVID-19 national and public health emergencies May 11 — signaling an end to the pandemic’s crisis era and an unwinding of federal flexibilities that reshaped the nation’s healthcare system.
“At present, the administration’s plan is to extend the emergency declarations to May 11, and then end both emergencies on that date,” the Office of Management and Budget said in a Jan. 30 statement. “This wind-down would align with the administration’s previous commitments to give at least 60 days’ notice prior to termination of the PHE.”
Over the last three years, the PHE has played a significant role in its influence of national healthcare policy — it reformed telehealth and expanded who can use it, fast-tracked approvals of COVID-19 vaccines and treatments, and preserved healthcare coverage for millions of Medicaid beneficiaries nationwide. HHS has renewed the PHE every 90 days since January 2020, with the most recent renewal declared on Jan. 11.
Though states could not disenroll people from Medicaid during the PHE, Congress passed a $1.7 trillion omnibus spending bill in December that detached the federal policy from Medicaid redeterminations. Starting April 1, states will begin redetermining who is and is not eligible for Medicaid, a process that could leave up to 18 million people without health coverage over the span of about a year.
The spending bill also extends Medicare telehealth flexibilities through 2024, which previously would have ended 151 days after the PHE expired. Acute hospital care at home waivers and flexibilities were also extended for two years through 2024. Similar to telehealth, the deadline for hospital at home waivers was tied to the status of the PHE. More than 250 hospitals have been approved by CMS to participate in the acute hospital care at home program.
COVID-19 tests and vaccines were covered for most Americans at no cost during the PHE, but the federal government has planned to shift much of these costs to the commercial market in 2023. Once the PHE ends, Medicare enrollees will generally face out-of-pocket costs for at-home tests and treatments, but vaccines would largely remain free for those with Medicare, Medicaid and commercial insurance. Medicaid programs will still cover physician-ordered tests, but treatments will incur a fee — commercially insured individuals can receive free treatments until federal supplies run out.
Commercialization would also leave the over 26 million uninsured individuals in the U.S. with a major disadvantage in accessing free vaccines and treatments. Moderna and Pfizer have floated commercial vaccine prices of up to $130 per dose.
The PHE’s termination will also mean states will no longer be required to report COVID-19 data to the CDC. A senior official with the Biden administration told ABC News that the CDC will be reaching out over the next few months to urge them to continue sharing data voluntarily.
News of the declaration’s tentative end comes as the flu, COVID-19 and respiratory syncytial virus — which have strained hospitals for months — appear to have peaked. In September, President Joe Biden declared the pandemic “over” amid a decline in case totals and deaths.
“It’s been a heavy flu season and a significant time for other illnesses,” Chip Kahn, president and CEO of the Federation of American Hospitals, toldBecker’s Jan. 11. “I do think we’re fast approaching a point where there will be heightened [COVID-19] surges, but this will be part of the routine — it’s becoming integrated with hospital activity, especially with the drugs and treatment knowledge at this point.”
On Jan. 30, the World Health Organization determined COVID-19 remains a public health emergency while also acknowledging the pandemic is “probably at a transition point.” The WHO’s emergency committee recommended the agency work with stakeholders on a proposal for how to maintain focus on COVID-19 once its emergency declaration is terminated.
Eleventh-hour financial improvements were not enough for U.S. hospitals, making 2022 “the worst financial year for hospitals and health systems since the start of the COVID-19 pandemic,” according to Kaufman Hall.
The declaration is hardly a surprise as hospitals’ median monthly margins lingered in the red throughout the first 11 months of 2022, starting with the -3.4 percent recorded in January, driven by the omicron surge. December was the only month where hospitals realized a positive year-to-date operating margin at 0.2 percent, according to Kaufman Hall’s latest “National Flash Hospital Report” — based on data from more than 900 hospitals.
Approximately half of U.S. hospitals finished the year with a negative margin, Kaufman Hall reported.
Labor expenses were a constant source of pressure throughout the year, with both a competitive labor market and greater reliance on more expensive contract labor to meet staffing demands driving hospital expenses that their bottom lines could not outdo, even with increased patient volumes.
Hospital labor expenses grew by 2 percent from November to December, and total direct expense per provider FTE grew to $592,430 in the fourth quarter of 2022, a 5 percent increase compared to the fourth quarter of 2021.
“As we saw throughout 2022, the labor market was unkind to hospitals and provider groups,” Erik Swanson, senior vice president of data and analytics with Kaufman Hall, said. “Given that labor and non-labor expenses are unlikely to recede in 2023, hospitals can embrace better workforce management strategies and leverage their relationships with post-acute care settings to maximize current patient volume trends.”
The analysis also found hospitals experienced increased patient volumes, particularly in outpatient settings as the front door of the hospital shifted away from the emergency department and toward ambulatory and outpatient surgical settings. The net patient revenue per provider FTE rose to $397,493, an 8 percent increase year over year.
“The pandemic fueled a fundamental shift in how patients are choosing to access their routine care,” Matthew Bates, managing director and physician enterprise service line lead with Kaufman Hall, said. “Providers are seeing more patients than ever, particularly in primary care settings, and care is moving away from hospitals. Medical groups should seek to improve individual provider productivity and efficiently integrate advanced practice providers to meet the increase in volume and successfully bend the cost curve.”
Eight drugmakers together have 21 oseltamivir presentations — a common flu drug sold under the brand name Tamiflu — on back order and allocation, and most cannot estimate a resupply date, according to the American Society of Health-System Pharmacists.
Most drugmakers did not share with ASHP a reason for the shortage, but one cited the supply issue as a reason for high demand. The shortage of the common flu drug is not national, according to the FDA, but some local pockets are noting increased demand and shortages.
Here’s how the oseltamivir shortage breaks down as of Jan. 11, per ASHP:
Alembic Pharmaceuticals has one presentation on back order with a resupply date of late January and two others on allocation.
Amneal Pharmaceuticals has four oseltamivir products on back order.
Camber Pharmaceuticals has three on allocation.
Lupin Limited has four on allocation.
Macleods Pharma has one on back order with a release date of early February and another on allocation.
Novadoz has three on allocation.
Teva Pharmaceuticals has one on intermittent back order and is resupplying as product becomes available.
Hospitals experienced a slight boost to operating margins in November, but not enough to restore the median negative margins that persisted for 2022 to date.
Kaufman Hall’s December “National Flash Hospital Report” — based on data from more than 900 hospitals — found hospitals’ median operating margin was -0.2 percent through November, a slight improvement from the median of -0.3 percent recorded a month prior.
A 1 percent decline in expenses from October to November drove the eleventh-hour improvement to margins and tipped the scales on hospitals’ relatively flat revenue. Additionally, hospitals saw labor expenses decrease 2 percent in November, potentially driven by less reliance on contract labor.
The median -0.2 percent margin recorded in November 2022 marks a 44 percent decline for margins in 22 year-to-date compared to 2021 year-to-date. Kaufman Hall’s index shows hospitals’ median monthly margins have been in the red throughout 2022, starting with the -3.4 percent recorded in January, driven by the omicron surge. November is tied with September as hospitals’ best month of the year, with both sharing a median margin of -0.2 percent.
Outpatient care marks one of the brighter spots for hospitals’ finances, with outpatient revenue up 10 percent year-over-year while inpatient revenue was flat over the same time period.
“The November data, while mildly improved compared to October, solidifies what has been a difficult year for hospitals amidst labor shortages, supply chain issues and rising interest rates,” Erik Swanson, senior vice president of data and analytics with Kaufman Hall, said. “Hospital leaders should continue to develop their outpatient care capabilities amid ongoing industry uncertainty and transformation.”
The number of amoxicillin products on back order has increased to 44 after months of the antibiotic being out of stock, according to the American Society of Health-System Pharmacists.
Depending on the ASHP’s website or the FDA’s drug shortage database, between two dozen and three dozen oral presentations of amoxicillin have been in shortage because of high demand since late October. At the time, the shortage was expected to resolve by the end of 2022.
As of Dec. 8, most drugmakers told ASHP they could not estimate a resupply date, but Teva Pharmaceuticals has release dates in January and February, and Hikma Pharmaceuticals short-dated their allocated supply for August 2023.
The worsening supply issue could be connected to the surge in viral infections even though amoxicillin is not a recommended treatment for COVID-19, flu or respiratory syncytial virus infections. Amoxicillin is not recommended to treat RSV cases, but some physicians will prescribe antibiotics when they are not medically necessary.
The original drug shortage may have sent a ripple effect through amoxicillin/clavulanate products — the recommended backup treatment for some infections if amoxicillin is not available — because 29 of them were in short supply as of late November.
From tracheostomy tubes and syringes to amoxicillin and dozens of other drugs, medical supply chains are hindered by ongoing issues to access raw materials and enough staff, The State Journal reported Dec. 4.
“I’ve been doing this [for] about 25 years,” Bryan LaBuda, WVU Medicine director of enterprise materials management, told The State Journal. “I would say this is unprecedented. Obviously, there’s always back orders and things like this, but in my career I’ve never seen the volume and the variety of back orders. That’s 100 percent due to the pandemic, which turned into labor shortages, as well.”
Other hospital supply chain leaders have lamented the labor shortage and higher prices for raw materials, which are more scarce partly because of inflation and partly because of geopolitical frictions.
Mr. LaBuda told The State Journal one way to counteract the persistent issues are “strategic vendor partnerships that have a focus on domestic manufacturing” — a growing trend called nearshoring and friend-shoring. WVU Medicine is also building its own distribution center to combat future supply chain hiccups.
As the “tridemic” of flu, COVID-19, and respiratory syncytial virus continues, pediatric hospitals are running into a new problem: a shortage of medical-grade cribs, CNN reported Dec. 5.
Grand Rapids and Southfield, Mich.-based Corewell Health ordered more than 50 cribs and have brought out both specialized and non-specialized cribs from storage to meet the demand of patients, hospital officials told CNN.
They aren’t the only ones struggling to meet demand.
“These shortages vary from items being on backorder with no estimated shipping date to product discontinuation without notice. The reasons include transportation issues and labor shortages,” Cynthia Zheng, director of pharmacy operations and support services at Wilmington-based Nemours Children’s Health Delaware Valley, said in the report. “At Nemours Children’s Health, these supply challenges are magnified due to pediatric populations needing more specialized equipment to accommodate different stages of growth. In addition, the high volumes as a result of an early spike in RSV have only put more strain on an already stressed system.”
Ventilators are also in high demand due to the RSV surge. CNN reported that the American Hospital Association said it received its first non-COVID-19-related request to the dynamic ventilator reserve since its launch in April 2020.